Diabetes is the most common chronic, serious ailment in the US. It is the main contributor to renal failure and blindness. It may result in amputations due to nerve injury. And diabetes dramatically raises the risk of heart disease and stroke. Despite the broad swath of diabetes cuts through our society, many people harbor misconceptions about the disease.
- Misconception #1: Diabetes is a disease that affects children; if you do not have it, you do not need to be concerned.
- Misconception #2: Diabetes is an older adult’s disease, and middle-aged people needn’t worry about it.
- Misconception #3: When older people get diabetes, it’s mild.
TWO TYPES OF TROUBLE
Elevated blood sugar levels and improper protein and fat metabolism are features of both types of diabetes.
- Diabetes Type 1 manifests most frequently by early adulthood, but only 5% to 10% of diabetic patients have this variety, formerly known as juvenile-onset diabetes.
- Diabetes Type 2 strikes 8% to 10% of adults at some time in their lives. Half of those with the disease do so before age 60, despite Type 2 typically appearing after age 45.
Background: Normally, insulin, an enzyme synthesized by beta cells in the pancreas, regulates blood sugar.
In type 1 diabetes, an auto-immune reaction destroys the beta cells, leaving the body unable to make insulin. Without insulin injections, death may occur in a manner of days.
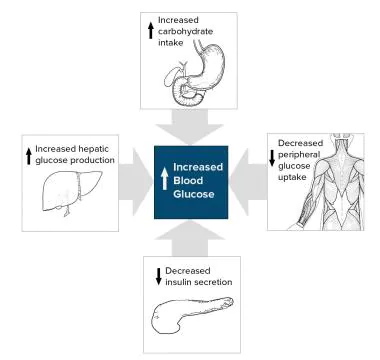
In type 2 diabetes, which frequently associates with obesity, beta cells fail to produce enough insulin resulting in a combination of insulin resistance, insufficient insulin secretion, and excessive or inappropriate glucagon secretion. Because Type 2 diabetics may not require insulin shots, many people mistakenly believe the disease isn’t severe.
Type 1 diabetes typically manifests quickly as complaints of extreme thirst, frequent urination, blurred vision, or unexplained weight loss.
With Type 2, glucose levels rise so slowly that symptoms appear later or develop so gradually that they show up only after complications occur.
Type 2 diabetes accounts for half of all cases, with half of those affected being overweight and utterly unaware of their condition. Furthermore, the more prolonged diabetes is untreated, the more likely complications are.
TESTING GUIDELINES
The following indications are included in diabetes screening in asymptomatic adults:
- Sustained blood pressure greater than 135/80 mm Hg
- Overweight and one or more other diabetes risk factors (e.g., first-degree relative with diabetes, blood pressure >140/90 mm Hg, HDL 35 mg/dL, and/or triglyceride level >250 mg/dL)
- In the absence of the criteria mentioned above, the ADA recommends screening at the age of 35
The recommended screening test is more straightforward and less unpleasant than the oral glucose tolerance test. After an overnight fast, the patient has a sweet syrup to drink, followed by a blood test two hours later.
The fasting plasma glucose test also requires an overnight fast. But the patient doesn’t have to drink the sweet liquid or wait two hours.
With the old guidelines, anyone whose fasting blood sugar level was 140 or higher or whose sugar level two hours after the drink was 200 or higher had diabetes.
With the current guidelines, the cutoff is 126. Research shows that complications develop when blood sugar rises above that level.
Whether a hemoglobin A1c (HbA1c) level of 6.5% or higher should be considered a primary diagnostic criterion or an optional one is debatable.
GETTING THE BEST TREATMENT
From diet and exercise to new drugs, there are several ways to control type 2 diabetes and associated problems like high blood pressure, elevated triglycerides, low HDL (good) cholesterol, etc.
If detected early, type 2 diabetes can often be controlled with diet and exercise alone.
Eighty percent of type 2 diabetes are overweight. Once these patients lose weight, even as little as a few pounds, their blood sugar level and metabolic state improve, and so do blood pressure and cholesterol levels.
Unlike diabetes Type 1, who must carefully monitor the balance of carbohydrates to other foods at every meal, diabetes Type 2 can mainly concentrate on cutting calories.
The best method to accomplish this is to reduce saturated fat while increasing the consumption of grains, fruits, and vegetables.
What about eating less sugar? That’s less important for Type 2 than Type 1 diabetics. However, since reducing sugar consumption can help keep blood sugar under control, it’s worth doing.
Exercise reduces the body’s insulin needs by boosting the cells’ sensitivity to insulin. To begin, take a 20-minute evening walk or take the stairs instead of the elevator at work, while shopping, etc.
Caution: If you aren’t used to physical activity, check with your doctor first.
When diet and exercise aren’t enough to do the job, it’s time for drug therapy. There are now a variety of medications that can help control type 2 diabetes.
- Sulfonylureas (SFUs) stimulate the pancreas to make insulin. Side effects can include hypoglycemia (low blood sugar) and weight gain.
- Biguanides, including metformin (Glucophage), reduce the amount of sugar released by the liver. This lower blood sugar to levels similar to those achieved with SFUs but without the side effects of hypoglycemia or weight gain.
- Alpha-glucosidase inhibitors, including acarbose (Precose), slow the digestion of carbohydrates and block their absorption. Because their effect on blood sugar isn’t as powerful as SFUs and biguanides, these medications are generally better suited for mild diabetes.
- Thiazolidinediones, including rosiglitazone [Avandia]) act as insulin sensitizers, requiring the presence of insulin to function. To be effective, they must be taken for 12-16 weeks.
INSULIN INJECTIONS
When oral drug therapy fails to control diabetes fully, insulin injections can dramatically lower glucose levels. Most patients who learn to give themselves insulin injections are surprised at how simple and painless the process is.
Diabetes Type 2 rarely requires the frequent injections needed to control Type 1 once or twice a day is often enough.